Why I am betting on invasive BCI
The short answer is this:
- We do not want visible devices. No electrodes all over the face. No headsets.
- We want true thought. That means inner speech.
- Any advances that make non-invasive possible make invasive 100x better.
More detail below.
I started River to solve one problem. The channel between thought and machine is lossy. Typing is the crudest version of it; fast, layered thought forced out clumsily through ten fingers, one character at a time. As AI made language the default interface to computers, voice AI has seen a resurgence. But it too has privacy issues, and background noise drives up error. You see tech bros in SF whispering into microphones to control their agents. It already feels like we're watching a relic, and we're just a few months in.
What we really want is to have our thoughts directly translated into intent, feeling and text, without the lousy motor and keyboard pathway, or verbal expression which is rate limited and prone to deterioration by disease, age and disorder.
And none of the devices today give us that. Neuralink inserts electrodes into the brain and leaves damage that doesn't fully heal. Would you put that into someone you love, unless they were dying and the little speech or mobility it bought them was worth the time they had left? Sabi and AlterEgo are building non-invasive devices and have great marketing campaigns on X, but the reality is that they require laborious attempted speech, which is essentially speaking with your mouth closed. This is not really thought. When you think, do you consciously mouth the words? No.
Axioms by which to judge BCI
While we know what we want out of BCI, it is helpful to assess the technology against some framework. The way I have approached this is laid out below.
First, you do not want to spend hours collecting training data.
Second is the form factor. Let's take EMG as an example of what you don't want, which is electrodes all over your face. That's too invasive. You want something like a headphone or behind the ear. Ideally, you don't want anything visible!
Third is true thought decoding. Most non-invasive technologies, and even some invasive, do attempted speech. The best way I can describe it is close your mouth and whisper something moving your tongue, larynx and cheek muscles, just without making a sound. That's attempted speech. It doesn't feel natural, though can be learned like typing. But it's still not what we consider to be thought.
Fourth is accuracy and speed. I lump the two together, though they are distinct. These two metrics are assessed as WPM (words per minute) and WER (word error rate).
Fifth, and most important, is invasiveness. Alter the anatomy as little as you can. Cut and embed no more than you have to, leave no lasting damage, and above all, do not kill or damage neurons as a side effect.
Why we did not pursue non-invasive routes
I really want non-invasive to work. The idea of it is appealing, though I am convinced 95% of these ideas are tar pits, because you simply can not argue with the physics to achieve the end goal.
Let's look at some of the the impressive companies in this space.
Apple bought Q.ai (presumably for their patent portfolio), which uses visual imaging of the cheek to decode some words, and I believe their intention is to integrate this into AirPods. But its performance varies in different lighting conditions, and I don't know if a demo has been published.
Sabi - show me the science. Everyone has tried EEG, and in the section below, I explain why I don't think it will work as promised.
AlterEgo - I don't buy the demo. The device is a Bluetooth-headset form factor sitting behind the ear, with a small contact just in front of the ear. The problem is anatomical. That preauricular contact does NOT overlie the muscles that carry phoneme-level information. Those are all anterior/inferior and well outside that contact's pickup radius. Too many questions to be answered. So at best that location yields coarse jaw EMG comprised of an open/close envelope and rough timing, a few bits.
The best one is in stealth. I am not at liberty to describe how it works, though I can say I was conversational in 5 minutes, and immediately thought "Damn, I might be working on the wrong thing". It doesn't quite solve the problem, because it's not really reading thought. And if you have some disorder that affects your efferent signal chain such as aphasia, ALS, or brainstem stroke, this device, and all other non-invasive devices that read motor signals instead of the originating cortical-level signal, will be unsuitable for you.
Various modalities, tried and abandoned
I've worked with almost every non-invasive modality you can think of, starting with EMG and EEG.
EMG reads the electrical signature of muscle fibres firing, the motor unit action potentials at the tail end of the efferent chain, well after cortex has issued the command. It wants electrodes all over your face. So it fails on form factor, and on thought, before you even begin. We still gave it a fair shot. We made our own electrodes from PEDOT:PSS, a conjugated polymer I'm fond of, combined with polydopamine, which is the chemistry mussels use to cling to wet rocks, so they'd stick to damp surfaces like skin. They came out soft and comfortable, and they were lovely. The face did not care for electrodes all over it.
The EEG form factor could be attractive, but the best decoding today is usually motor or binary intent (yes/no) because anatomy gets in the way. The skull is fifteen to eighty times more resistive than the brain tissue beneath it, so by the time a cortical signal reaches the scalp it has lost roughly an order of magnitude in amplitude and been smeared across centimetres of skin (McCann et al., 2019). You need something like 6 cm² of cortex firing in lockstep before signal even shows up at a scalp electrode (Cooper et al., 1965). Worst of all, the skull hits high frequencies hardest. The 70 to 170 Hz high-gamma band that speech decoding depends on is so attenuated that scalp EEG in that range is mostly picking up muscle, not brain (Ball et al., 2009). That muscle signal is decodable, but it's not thought.
Then we considered optical sensing. The brain consumes energy, and when a region becomes active it needs to be replenished with blood, so optical sensing measures the change in blood oxygen as this happens. We abandoned it for a few reasons. First, sealing the light is tricky. You can't have light leaking in between the transmitter and the skin, or leaking out, and for anyone with hair, and everyone who is mobile, that is a hard problem. There's also the fact that light is fundamentally an energy transfer mechanism, which almost no one talks about. Photons displace nitric oxide from cytochrome c oxidase, a protein in your mitochondria, which frees up oxygen to bind at the iron and copper centre of complex IV and act as the terminal acceptor for electrons. This drives the electron transport chain, which builds the proton gradient that synthesises ATP from ADP (tri from di) using spare phosphate. The net effect is whichever region is exposed to photons has more energy, and is a well-studied mechanism in neuroplasticity treatments. You are no longer just measuring the brain, you are changing it. That's invasive.
None of these devices clear all five axioms. Even with data scaling laws on our side, we could not solve the problem we wanted to solve without going inside. So I bet on invasive.
The state of Invasive
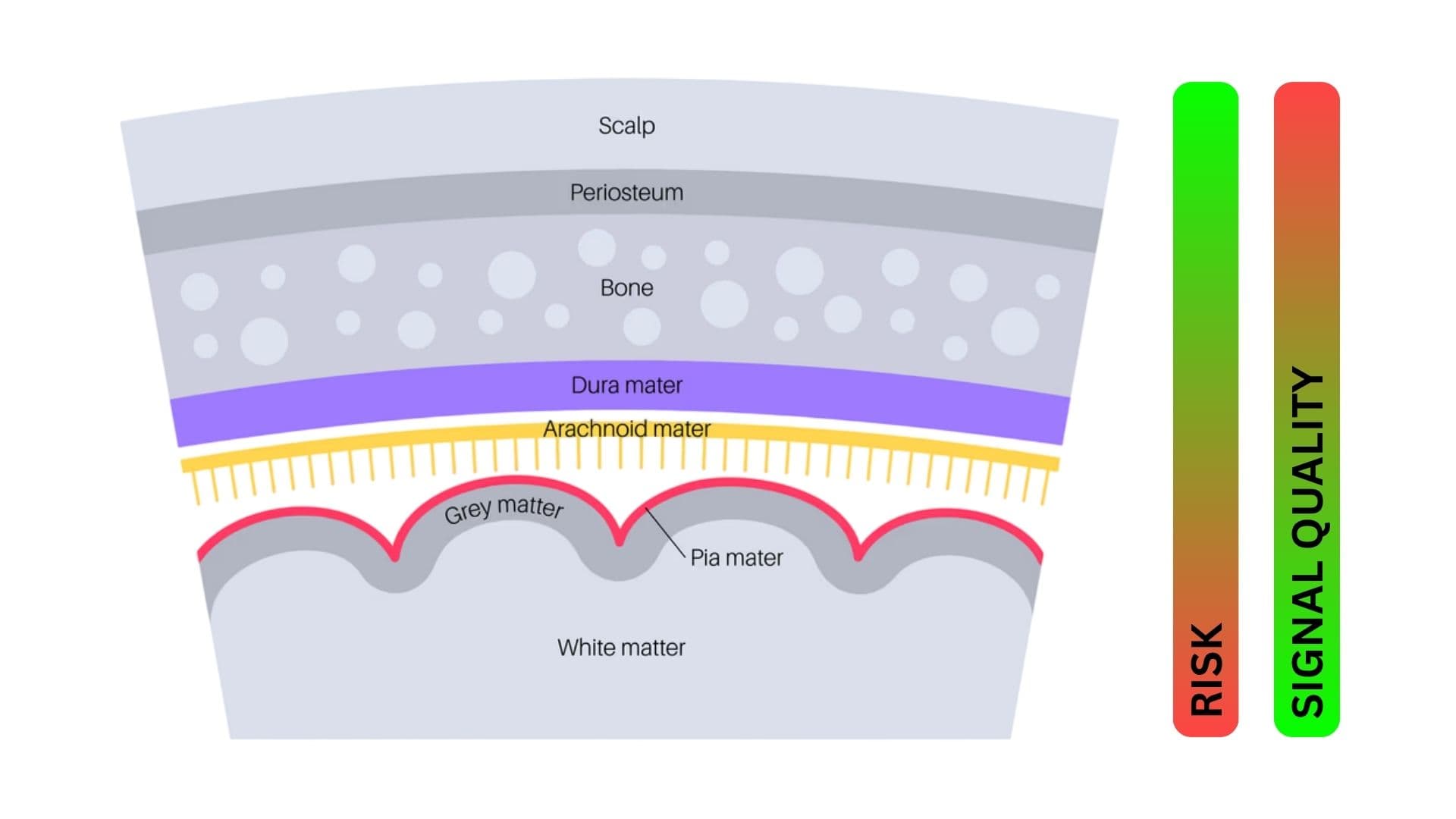
The invasive game is one where you trade off risk and damage for signal quality.
Intracortical
Intracortical unequivocally has the best signal quality. You can detect activity of single neurons! That is amazing, and what you can do with it is nothing short of miraculous on both the read-out and write-in modalities.
However, the risks are severe. Firstly, there is gliosis. When you put foreign material into the body, the immune system attacks it. Microglia and astrocytes flock to the site, building up a protective layer around the shank. This degrades signal quality (Polikov et al., 2005).
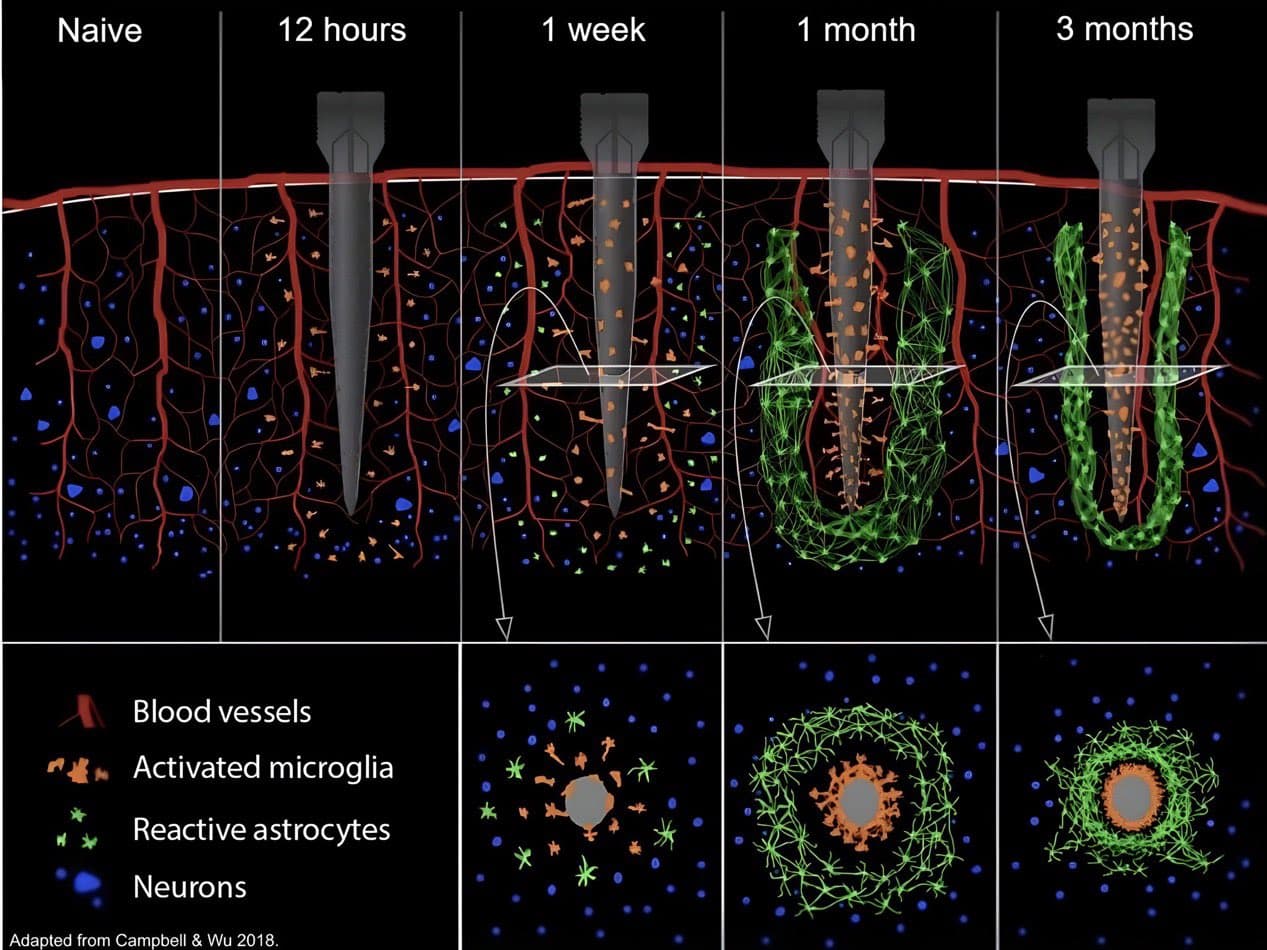
Then there's micromotion. The brain is soft and never sits still. With every heartbeat it shifts two or three microns against a rigid shank, and every breath moves it another ten to thirty microns (Gilletti & Muthuswamy, 2006). That sounds tiny until you remember it happens around 100,000 times a day, every day, for the life of the implant. In rigid arrays like the Utah array and Paradromics' microwires, this constant grinding of a stiff probe against soft tissue keeps the wound inflamed, and it is part of why the signal fades over the years. Around each shank the cortex is left with a dead zone of neurons roughly 100 to 150 microns across (Biran et al., 2005), and adult cortex does not regrow them, so the damage is permanent.
Neuralink deserves a caveat. Its threads are not rigid shanks but ultra-thin flexible polymer, and that helps. In animals, soft, low-footprint probes that move with the brain rather than against it provoke far less scarring and preserve far more neurons than rigid ones (Zhou et al., 2017). But flexibility softens the problem, it does not erase it. You still have to push the thread in, and the insertion, plus the body's lifelong response to a foreign object, leaves damage. Neuralink's thin-film threads also sit closer to the ordinary flexible probes that scar than to the softest mesh that barely does, and there is no published human histology for them yet. So the fair read is that flexible threads reduce the damage, not that they remove it, and in a living person we do not yet know by how much.
In rats, intracortical probes measurably degrade fine-motor capability. In one study, implanted rats took up to 527% longer to complete a fine-motor task than controls, and the deficit was still there at 16 weeks (Goss-Varley et al., 2017). In humans, this is harder to measure, because the probes cover a smaller percentage of the brain than in rats, and because most patients so far have had serious paralysis already. How do you measure how much motor movement is lost in a paralysed patient?
Now, knowing what you know, whether that's a lot of neuroscience or just what you've read here, would you want intracortical electrodes from Neuralink, Paradromics, or anyone else put into yourself or someone you love? Only, I think, if they were in the last few years of an incurable disease like ALS.
Synchron and the endovascular paradox
Synchron is beautiful. It is the paragon of "work with evolution, not against it". There is no craniotomy, it is far less invasive than anything that opens the skull, and the scaffold is built to last a lifetime.
On the business side, there are already thousands of people in hospitals around the world called neurointerventionists who perform these procedures to unblock arteries during stroke. These are high pressure situations where the procedure must be decided for and performed quickly to save a life, and they are often highly effective with minimal complications. Synchron achieved instant distribution with a very safe and effective device that works with the body. You can't fault it.
There are a few key limitations to Synchron though.
Firstly, it only has 16 channels, so people use it as a rudimentary motor control device (Oxley et al., 2016). That can be changed, I imagine, and it would be unsurprising if Synchron is soon at 512 or even 1024 channels.
The main problem with Synchron is anatomy. To decode speech you need access to the ventral premotor and sensorimotor cortex (area 6v) (Bouchard et al., 2013) and parts of Broca's area. You can also pull decodable signal from the supramarginal gyrus, as Wandelt did (Wandelt et al., 2024), and from the superior temporal gyrus (Chang et al., 2010). These all sit out on the lateral surface of the brain. The Stentrode works because the superior sagittal sinus is a large, safe vein running right over the midline motor strip, but the lateral speech areas have no equivalent highway. Their arterial supply, the middle cerebral artery and its branches, is far smaller than the sagittal sinus, and the superficial cortical veins that drain them are small, tortuous, and vary a lot between people. There is no big, reliable vessel sitting over Broca's area the way the sagittal sinus sits over motor cortex.
There are zero in-vivo arterial endovascular BCI studies, and for good reason. The cortical arteries feeding the speech areas are small, and a permanent electrode-covered stent parked in one risks occluding the vessel and the tiny perforators branching off it, starving the cortex you are trying to read and causing an ischemic stroke. That is what these devices are ordinarily trying to prevent!
So Synchron, awesome. But it is not able to solve the problem, probably no matter how much they innovate. I hesitate to say never, but it's improbable due to the risks of leaving permanent stents in arteries.
The surface
Decoding from the cortical surface has a long history of being safe and effective. Edward Chang at UCSF is the leading researcher in this field, having conducted multiple in-human trials. To my knowledge, the Chang lab is the only group with chronic, multi-year, large-vocabulary data in paralyzed humans through their BRAVO trials.
Moses et al. demonstrated the first closed-loop ECoG speech BCI with a 128-channel grid in an anarthric stroke survivor, achieving 25.6% WER on a 50-word vocabulary at 15.2 WPM (Moses et al., 2021).
Metzger et al. extended this with a 253-channel array in a second participant, reaching ~25% WER on a 1,024-word vocabulary at 78 WPM, with simultaneous text, synthesized voice, and avatar output from attempted silent speech (~21% pre-LM phone error) (Metzger et al., 2023).
Silva et al. showed the neural representations remained stable for years on the same array (Silva et al., 2024), and Littlejohn et al. added streaming brain-to-voice synthesis at 46.5 WPM with ~30.7% WER (Littlejohn et al., 2025).
All of Chang's research was conducted with PDMS (polydimethylsiloxane, aka silicone) arrays. But silicone is incompatible with high density designs because it interacts poorly with photolithography, leading to wider pitch (spacing between electrode contacts). In Chang's example, the pitch was 4 mm.
High-gamma activity in human cortex has a spatial decorrelation length of ~1.4 mm, so Chang's 4 mm pitch undersamples by roughly 3× per dimension, as demonstrated by Muller et al. (Muller et al., 2016). Tighter pitch decodes better. Sub-2 mm gives 35% better decoding and 48% higher SNR, and under 2 mm is the threshold for reaching 95% of full-array performance, as shown by Duraivel et al. (Duraivel et al., 2023). And the gains don't saturate. A 1,024-channel array at 400 µm pitch keeps climbing in accuracy with channel count, with no sign of a plateau, as demonstrated by Hettick et al. (Hettick & others, 2025). The takeaway is that tighter pitch and more channels keep paying off, they don't plateau. I've spared you the full spatial-frequency analysis here. If you want it, get in touch and ask for River's data room.
So we know that even with a coarse pitch, we can get to 78 words per minute and a 25% word error rate on a large vocabulary, and that tightening the pitch increases spatial resolution and decoding accuracy significantly. Great.
Now this brings us to the key problem, and it is a materials tradeoff. PDMS lasts a long time in the body, but as we saw it can't do fine pitch. Polyimide is the opposite. It's compatible with standard lithography, so you can get very fine pitches down to single-digit microns, but it doesn't last, and that is inherent to its chemistry.
BPDA/PDA polyimide (biphenyl dianhydride / p-phenylenediamine) is formed by thermal imidization of a polyamic acid (PAA) precursor. During curing, two water molecules are expelled per repeat unit as the imide rings (–CO–N–CO–) close.
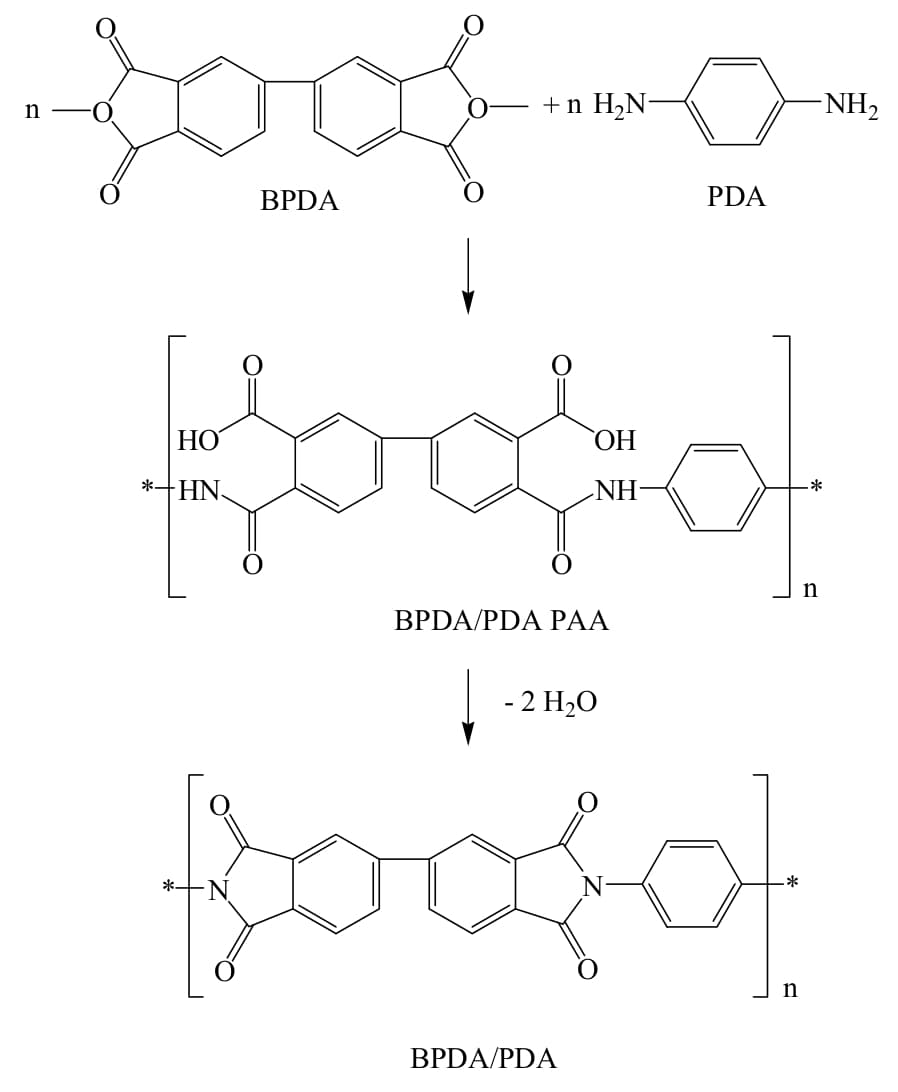
In a chronic physiological environment, this condensation reaction is reversible. Water molecules present in interstitial fluid attack the electrophilic carbonyl carbons of the imide ring, cleaving the C–N bond and reopening the ring structure. This hydrolysis swells the polymer matrix, generates internal stress at buried interfaces, and weakens adhesion between encapsulation layers and underlying metal traces.
BPDA/PDA is among the better-performing polyimides in this regard. Bulk water absorption at saturation is approximately 1 wt%, lower than most alternatives in the polyimide family. However, saturation is reached within 3 days of saline exposure at body temperature. Moisture absorption in polyimide films follows Fickian diffusion kinetics and scales nearly linearly with relative humidity across the operating range, meaning there is no threshold below which absorption ceases. Once implanted, a polyimide device is absorbing from day one.
This relationship between water absorption and compatibility with high-density manufacturing processes is one of the major reasons that chronic, high-density surface arrays have been the exception, rather than the norm.
River uses a new material (that we patented, but I am not ready to talk about yet) that has very tightly packed molecular bonds, and thus, a very low water absorption rate, even lower than parylene C (0.06 wt%), which is what the field generally uses to keep moisture out. It's compatible with high-density manufacturing processes, is easy to obtain, and quite forgiving to work with.
The science is proven, and the last piece of the puzzle is now a solved problem. With the exception of stimulation, surface decoding already gives you conversational-rate speech. While intracortical looks better on paper, surface gets there without the gliosis and chronic inflammation that make Neuralink and its intracortical cousins so repellent.
Come back to the five axioms. Surface decoding is close to clearing all of them. Setup is a one-time procedure, not hours of daily calibration. The form factor vanishes under the skin, with nothing visible. The accuracy and speed are already there, 78 words per minute at a 25% word error rate, and climbing as the pitch tightens. It reads from the cortex itself, which is the only place true thought can ever be read from, rather than the muscle downstream. And on invasiveness, the one that matters most, it disturbs the least we can while still reaching real thought at conversational rate, resting on the surface, with no shanks pushed into tissue and no neurons killed to win the signal.
I see surface as the entry point, not the destination. The natural path from here is to keep working outwards, to epidural, giving up a little signal for even less risk, which I believe we can make up for with a large data bank and improvements in AI models beyond the GRU/CTC paradigm which dominates neural decoding.
Epidural
Reading from the cortical surface is safer than intracortical, but it is not risk free. We've evolved to have thick skulls and dura mater for a reason. I imagine it has something to do with the fact that organisms with little cerebral protection probably got infections or damaged their brains more easily, leading to lower survival rates. Does our evolutionary trajectory involve cutting into that now at scale? Probably not.
Epidural decoding can be done well. Acclaimed neuroscientist Sam John, who led most of Synchron's preclinical work and is now working with River on our preclinical studies, published a paper in 2018 with Tom Oxley showing the signal quality achievable at each level of invasion, finding endovascular, subdural and epidural recordings comparable (John et al., 2018) on some dimensions. Epidural decoding is entirely capable of capturing the high gamma signal band (70-170 Hz) which is so critical to speech decoding, but only IF the contacts are large (Bundy et al., 2014). This is known as macro-ECoG.
There are companies working on this modality, the most well-known of which are NEO in China (Hong & others, 2024) and WIMAGINE in France (Sauter-Starace et al., 2019) (Larzabal et al., 2021). They are incredibly elegant devices which remove a small bit of skull, but leave the dura and its CSF-sealing properties intact, and replace that section of skull with a titanium plate that has electrodes on one side. They work effectively and, on information, are safe enough to be considered for less-than-life-threatening conditions.
The first preprint for speech BCI was published on Arxiv in late December 2025, and the space is developing fast. Watch it.
Take Sabi, who promise to decode your thoughts and attempted speech from a beanie. It is unclear how. They have published nothing, no one has shown EEG doing this, and I am not aware of any published work using the hundred-thousand-sensor arrays they describe. But even granting their bet, the logic runs in our favour: if data scaling laws could ever pull reliable decoding from the skin, through the skull, then they should deliver a far better experience from epidural, where the signal is not fighting the skull at all.
This is why I am betting on invasive BCI. Over time, we'll find a way to "write in" to consciousness, ethically and in desirable fashion.
Then we can really say, "It's the thought that counts."
References
- McCann, H., Pisano, G., & Beltrachini, L. (2019). Variation in reported human head tissue electrical conductivity values. Brain Topography, 32(5), 825-858. doi:10.1007/s10548-019-00710-2
- Cooper, R., Winter, A., Crow, H., & Walter, W. (1965). Comparison of subcortical, cortical and scalp activity using chronically indwelling electrodes in man. Electroencephalography and Clinical Neurophysiology, 18, 217-228.
- Ball, T., Kern, M., Mutschler, I., Aertsen, A., & Schulze-Bonhage, A. (2009). Signal quality of simultaneously recorded invasive and non-invasive EEG. NeuroImage, 46(3), 708-716. doi:10.1016/j.neuroimage.2009.02.028
- Polikov, V., Tresco, P., & Reichert, W. (2005). Response of brain tissue to chronically implanted neural electrodes. Journal of Neuroscience Methods, 148(1), 1-18. doi:10.1016/j.jneumeth.2005.08.015
- Gilletti, A., & Muthuswamy, J. (2006). Brain micromotion around implants in the rodent somatosensory cortex. Journal of Neural Engineering, 3(3), 189-195. doi:10.1088/1741-2560/3/3/001
- Biran, R., Martin, D., & Tresco, P. (2005). Neuronal cell loss accompanies the brain tissue response to chronically implanted silicon microelectrode arrays. Experimental Neurology, 195(1), 115-126. doi:10.1016/j.expneurol.2005.04.020
- Zhou, T., Hong, G., Fu, T., Yang, X., Schuhmann, T., Viveros, R., & Lieber, C. (2017). Syringe-injectable mesh electronics integrate seamlessly with minimal chronic immune response in the brain. Proceedings of the National Academy of Sciences, 114(23), 5894-5899. doi:10.1073/pnas.1705509114
- Goss-Varley, M., Dona, K., McMahon, J., Shoffstall, A., Ereifej, E., Lindner, S., & Capadona, J. (2017). Microelectrode implantation in motor cortex causes fine motor deficit: Implications on potential considerations to Brain Computer Interfacing and Human Augmentation. Scientific Reports, 7, 15613. doi:10.1038/s41598-017-15623-y
- Oxley, T., et al. (2016). Minimally invasive endovascular stent-electrode array for high-fidelity, chronic recordings of cortical neural activity. Nature Biotechnology, 34(3), 320-327. doi:10.1038/nbt.3428
- Bouchard, K., Mesgarani, N., Johnson, K., & Chang, E. (2013). Functional organization of human sensorimotor cortex for speech articulation. Nature, 495(7441), 327-332. doi:10.1038/nature11911
- Wandelt, S., Bj\aanes, D., Pejsa, K., Lee, B., Liu, C., & Andersen, R. (2024). Representation of internal speech by single neurons in human supramarginal gyrus. Nature Human Behaviour, 8(6), 1136-1149. doi:10.1038/s41562-024-01867-y
- Chang, E., Rieger, J., Johnson, K., Berger, M., Barbaro, N., & Knight, R. (2010). Categorical speech representation in human superior temporal gyrus. Nature Neuroscience, 13(11), 1428-1432. doi:10.1038/nn.2641
- Moses, D., et al. (2021). Neuroprosthesis for decoding speech in a paralyzed person with anarthria. New England Journal of Medicine, 385(3), 217-227. doi:10.1056/NEJMoa2027540
- Metzger, S., et al. (2023). A high-performance neuroprosthesis for speech decoding and avatar control. Nature, 620, 1037-1046. doi:10.1038/s41586-023-06443-4
- Silva, A., et al. (2024). A bilingual speech neuroprosthesis driven by cortical articulatory representations shared between languages. Nature Biomedical Engineering, 8, 977-991. doi:10.1038/s41551-024-01207-5
- Littlejohn, K., et al. (2025). A streaming brain-to-voice neuroprosthesis to restore naturalistic communication. Nature Neuroscience. doi:10.1038/s41593-025-01905-6
- Muller, L., Hamilton, L., Edwards, E., Bouchard, K., & Chang, E. (2016). Spatial resolution dependence on spectral frequency in human speech cortex electrocorticography. Journal of Neural Engineering, 13(5), 056013. [Link]
- Duraivel, S., et al. (2023). High-resolution neural recordings improve the accuracy of speech decoding. Nature Communications, 14, 6938. doi:10.1038/s41467-023-42555-1
- Hettick, M., & others, . (2025). Minimally invasive implantation of scalable high-density cortical microelectrode arrays for multimodal neural decoding and stimulation. Nature Biomedical Engineering. doi:10.1038/s41551-025-01501-w
- John, S., et al. (2018). Signal quality of simultaneously recorded endovascular, subdural and epidural signals are comparable. Scientific Reports, 8, 8427. doi:10.1038/s41598-018-26457-7
- Bundy, D., et al. (2014). Characterization of the effects of the human dura on macro- and micro-electrocorticographic recordings. Journal of Neural Engineering, 11(1), 016006. doi:10.1088/1741-2560/11/1/016006
- Hong, B., & others, . (2024). Reclaiming hand functions after complete spinal cord injury with epidural brain-computer interface. medRxiv. doi:10.1101/2024.09.05.24313041
- Sauter-Starace, F., et al. (2019). Long-term sheep implantation of WIMAGINE, a wireless 64-channel electrocorticogram recorder. Frontiers in Neuroscience, 13, 847. doi:10.3389/fnins.2019.00847
- Larzabal, C., et al. (2021). Long-term stability of the chronic epidural wireless recorder WIMAGINE in tetraplegic patients. Journal of Neural Engineering, 18(5), 056026. doi:10.1088/1741-2552/ac2003